.png?width=300&height=69&name=SavvyCoop_HorizontalLogo_LargeFormat%20(1).png)
Last week my team had our (virtual) Quarter 3 planning retreat. We spent Day 1 listening, learning, and supporting each other through a targeted exercise, which we call the Hot Seat (better name TBD). Here’s how it went: one-by-one, each team member had the opportunity to share an area where they felt stuck or could use some feedback; this might be with a certain task, project, or even a personal habit. After they outlined the problem, others on our team had the opportunity to ask clarifying questions, but were NOT permitted to offer advice yet (believe me, it’s so tempting, and I regulated this pretty hard).

One team member shared that they were having a hard time staying on task and working efficiently. The natural reaction is to suggest to do lists, or block time on the calendar for specific tasks, but the problem was complex, and we needed more information in order to offer any meaningful suggestions.
The questions began to uncover that part of the problem they were facing about efficiency and staying on task revolved around the nature of their job, which entails timely responses to clients and patients. Through clarifying questions, our team learned they were beholden to their inbox notifications, making it near impossible to feel like they ever had stretches of time to focus. By asking questions first, we all saw the problem was not so easily solved.
The goal of the exercise is to understand the problem more fully before offering solutions. Only after we had exhausted questions and felt we had a gasp of both the vastness and intricacies of the problem did we finally go around and offer possible solutions.
What my team may not have known in the moment is that we were practicing exactly what Savvy stands for: don't assume you have solutions before you go straight to the source and meaningfully define the problem.
Defining the problem in healthcare
It’s human nature to jump in with solutions. And in an industry like healthcare, where I truly believe that people are generally trying to help, this can be even more pronounced. Yet, for all the solutions the healthcare sector proposes, more often than folks would like to admit, they may not have sufficiently defined the problem.
An example of this jumped out at me in a recently published article in the Harvard Business Review, entitled "Addressing Demographic Disparities in Clinical Trials.” Naturally, I was thrilled to see such a topic being spoken about outside of a health-specific forum, and in such a prestigious publication no less.
The authors share that the methodology for their framework was "based on interviews with dozens of leaders throughout the health care ecosystem, including disease foundation CEOs who participate in leadership forums hosted by the Harvard Business School Kraft Precision Medicine Accelerator."
The authors then went on to outline three potential solutions on how to increase diversity in clinical trials:
- Know what "representative” means for your disease and set intentional recruitment goals
- Use patient registry datasets as a basis for trials
- Go beyond traditional academic medical centers to access patients
While I don't disagree with these suggestions, I was left unsatisfied. That's because they went straight to solutions mode. They made the leap from “we need more diverse clinical trial participants” straight to “here’s how we fix it.”
There were no clarifying questions, like why are clinical trial participants not more diverse, how do different communities feel about clinical research, is it only clinical trials where this lack or representation exists, or what role does systemic racism play in this scarcity of diverse participants?
What to ask. Who to ask.
If we’ve learned anything from this past year, health disparities are rampant and there is no easy fix. It’s not that the proposed solutions were bad, they aren’t, but they do make a lot of assumptions. Here are some clarifying questions I would want to ask before proposing these solutions:
1. Know what "representative” means for your disease and set intentional recruitment goals
- Where do we get this information about prevalence and incidence rates? How do we know that data is accurate and doesn’t further reflect underdiagnosing in certain populations? Why might underdiagnosing in certain populations exist?
2. Use patient registry datasets as a basis for trials
- Are registries representative? Are they run by institutions or organizations that may also not be representative and reach diverse communities?
3. Go beyond traditional academic medical centers to access patients
- What is it about academic centers is the issue? The authors suggest several alternative places to recruit from (health systems, community networks, DTC marketing), but is the problem purely about access to diverse patients or is there more to explore there? I’ll come back to this...
And it's not just about asking the tough questions, but also being thoughtful about who you are asking. The authors shared that they interviewed "dozens of leaders throughout the health care ecosystem, including disease foundation CEOs." Again, that's fine, but did they only interview healthcare leaders? Will this perspective be representative across demographics and experiences, specifically race/ethnicity, sexual orientation, gender identity, socioeconomic status, and health literacy?
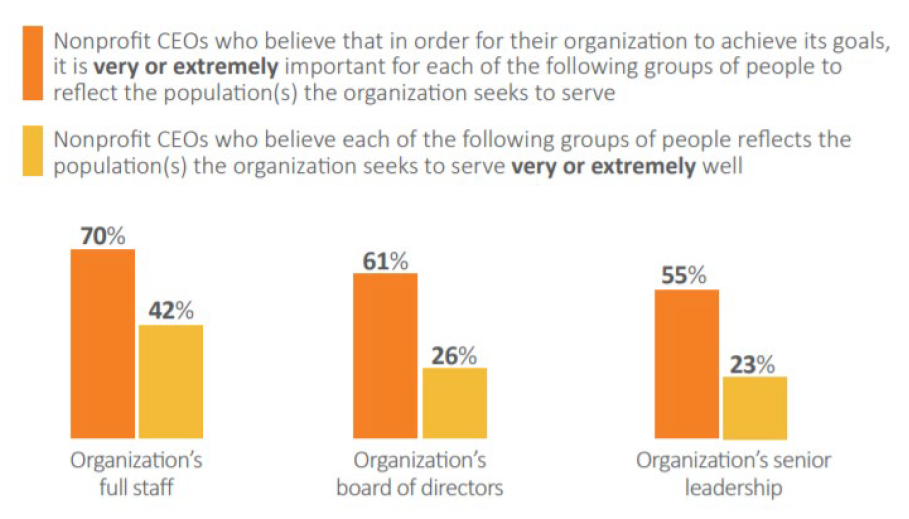
A 2018 study by the Center for Effective Philanthropy found that "despite 55 percent of nonprofit CEOs believing that it is “very” or “extremely important” for the senior leadership team to reflect the population the organization seeks to serve, only 23 percent believe their senior leadership team reflects the population they seek to serve “very” or “extremely well.""
Therefore, we need to ask ourselves if the people to which we ask these clarifying questions are the right people to define the problem in the first place?
• • •
Upstream vs downstream approach
When it comes to the behemoth challenge around clinical trial enrollment, this kind of advice seems too far downstream. Remember the Ever Given, the ship that got stuck in the Suez Canal for 6 days and required tugboats and dredgers to get it free? The incident caused a traffic jam of cargo ships that experts estimated held up nearly $10b of goods per day! A downstream approach (pun intended) would be to have more tugboats and dredgers on hand to help aid ships that run aground more swiftly. But you know that's not the solution...
It should feel more obvious that what really needs to happen is to ask how did we get here in the first place, with a real and metaphorical ship that is stuck and costing time and money with each day that passes.
We need to take a similar upstream approach when it comes to clinical trial enrollment. Simply trying to identify places to recruit diverse patients into trials, while important, seems to overlook how we got here in the first place and the historical injustices that have caused deep mistrust of clinical research within underrepresented communities.
At Savvy, we have done countless projects this past year alone to help unpack this core issue. Oftentimes, the client (e.g. a pharma company or CRO) generally comes to us with the problem “we need to enroll more diverse participants in our trial." One such client was Boehringer Ingelheim (BI), and to their credit, they wanted to do the work to understand the root of the problem. They were all-in to ask those tough clarifying questions to more fully understand how we got here.
We worked with BI to design a multiphase, multichannel, mixed methods approach where Savvy recruited and engaged patients representing Black, Indigenous, and people of color (BIPOC), Latinx, Hispanic, and Asian communities. You can read more about the first phase of the project here.
While BI came in with some hypotheses about what might help with enrollment, we first went deep with the participants to unpack their personal feelings and the cultural narratives about our healthcare system and clinical research before introducing possible solutions. Here is one such quote we heard:
“My grandfather told us about how they were allowed to go to the dentist. When you needed a tooth pulled you went to the veterinarian after midnight on a Sunday because people didn’t even want their animals to have the same medical care as black people.”
These problems are so complex, far more so than my colleague’s efficiency and task management challenges, and cannot be fixed until we truly understand the problem.
I'll give the authors of the HBR article the benefit of the doubt that they understand this too, but I think it warrants being called out. I don’t want to leave room for people to interpret such directives as a simple fix for an extremely complex problem.
When it comes to diversity, equity, and inclusion, we need to go to the source and ask thoughtful questions in order to fully understand how we got here, and then work with the community to co-design solutions that meaningfully address their needs.
In short, and as always, ask patients.
——————————————————
About Us
Jen Horonjeff, PhD, is a life-long autoimmune disease patient and brain tumor survivor turned human factors engineer, academic, FDA advisor, and now the founder & CEO of Savvy Cooperative.
Savvy Cooperative helps the healthcare industry create patient-centered products and solutions by providing a marketplace for patient insights. Pharma and startups alike can connect directly with patients to participate in clinical, UX, and market research. Savvy’s unique co-op model leverages its members’ networks to quickly recruit diverse patients, and pays patients for sharing their insights! Savvy’s award-winning co-op has been featured in FastCompany, TechCrunch, The Boston Globe, and named one of the 50 Most Daring Entrepreneurs by Entrepreneur Magazine.

